
Advertisement
-
Published Date
June 21, 2020This ad was originally published on this date and may contain an offer that is no longer valid. To learn more about this business and its most recent offers, click here.
Ad Text
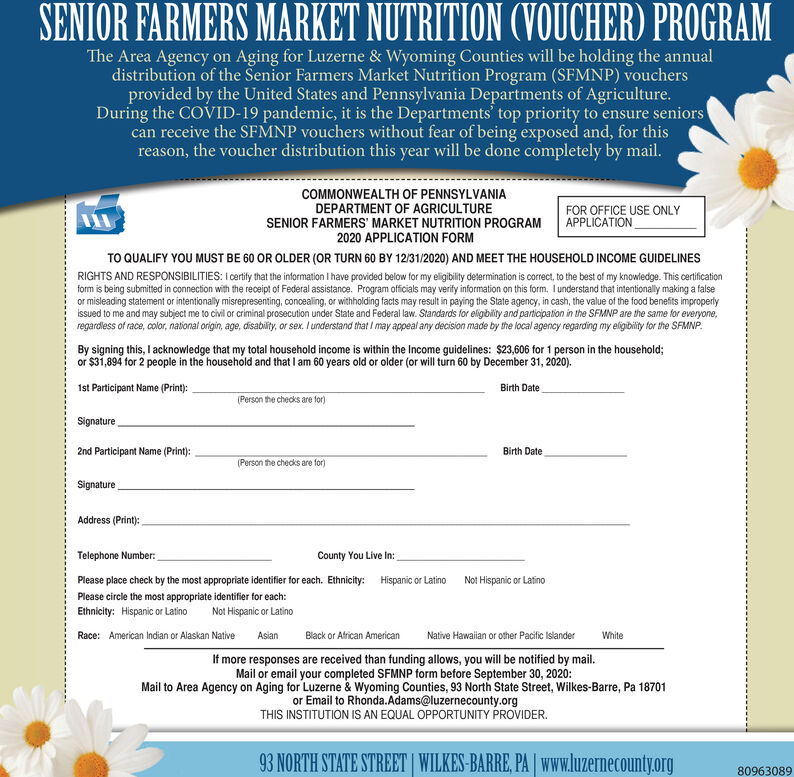
SENIOR FARMERS MARKET NUTRITION (VOUCHER) PROGRAM The Area Agency on Aging for Luzerne & Wyoming Counties will be holding the annual distribution of the Senior Farmers Market Nutrition Program (SFMNP) vouchers provided by the United States and Pennsylvania Departments of Agriculture. During the COVID-19 pandemic, it is the Departments' top priority to ensure seniors can receive the SFMNP vouchers without fear of being exposed and, for this reason, the voucher distribution this year will be done completely by mail. COMMONWEALTH OF PENNSYLVANIA DEPARTMENT OF AGRICULTURE SENIOR FARMERS' MARKET NUTRITION PROGRAM 2020 APPLICATION FORM FOR OFFICE USE ONLY APPLICATION TO QUALIFY YOU MUST BE 60 OR OLDER (OR TURN 60 BY 12/31/2020) AND MEET THE HOUSEHOLD INCOME GUIDELINES RIGHTS AND RESPONSIBILITIES: I certity that the information I have provided below for my eligibility determination is correct, to the best of my knowledge. This certification form is being submitted in connection with the receipt of Federal assistance. Program officials may verify information on this form, Iunderstand that intentionally making a false or misleading statement or intentionally misrepresenting, concealing, or withholding facts may result in paying the State agency, in cash, the value of the food benefits improperly issued to me and may subject me to civil or criminal prosecution under State and Federal law. Standards for eligibility and participation in the SFMNP are the same for everyone, regardless of race, color, national origin, age, disability, or sex. I understand that I may appeal any decision made by the local agency regarding my eligibility for the SFMNP. By signing this, I acknowledge that my total household income is within the Income guidelines: $23,606 for 1 person in the household; or $31,894 for 2 people in the household and that I am 60 years old or older (or will turn 60 by December 31, 2020). 1st Participant Name (Print): Birth Date (Person the checks are for) Signature 2nd Participant Name (Print): Birth Date (Person the checks are for) Signature Address (Print): Telephone Number: County You Live In: Please place check by the most appropriate identifier for each. Ethnicity: Hispanic or Latino Not Hispanic or Latino Please circle the most appropriate identifier for each: Ethnicity: Hispanic or Latino Not Hispanic or Latino Race: American Indian or Alaskan Native Asian Black or African American Native Hawaiian or other Pacific Islander White If more responses are received than funding allows, you will be notified by mail. Mail or email your completed SFMNP form before September 30, 2020: Mail to Area Agency on Aging for Luzerne & Wyoming Counties, 93 North State Street, Wilkes-Barre, Pa 18701 or Email to Rhonda.Adams@luzernecounty.org THIS INSTITUTION IS AN EQUAL OPPORTUNITY PROVIDER. 93 NORTH STATE STREET | WILKES-BARRE, PA Www.luzernecounty.org 80963089 SENIOR FARMERS MARKET NUTRITION (VOUCHER) PROGRAM The Area Agency on Aging for Luzerne & Wyoming Counties will be holding the annual distribution of the Senior Farmers Market Nutrition Program (SFMNP) vouchers provided by the United States and Pennsylvania Departments of Agriculture. During the COVID-19 pandemic, it is the Departments' top priority to ensure seniors can receive the SFMNP vouchers without fear of being exposed and, for this reason, the voucher distribution this year will be done completely by mail. COMMONWEALTH OF PENNSYLVANIA DEPARTMENT OF AGRICULTURE SENIOR FARMERS' MARKET NUTRITION PROGRAM 2020 APPLICATION FORM FOR OFFICE USE ONLY APPLICATION TO QUALIFY YOU MUST BE 60 OR OLDER (OR TURN 60 BY 12/31/2020) AND MEET THE HOUSEHOLD INCOME GUIDELINES RIGHTS AND RESPONSIBILITIES: I certity that the information I have provided below for my eligibility determination is correct, to the best of my knowledge. This certification form is being submitted in connection with the receipt of Federal assistance. Program officials may verify information on this form, Iunderstand that intentionally making a false or misleading statement or intentionally misrepresenting, concealing, or withholding facts may result in paying the State agency, in cash, the value of the food benefits improperly issued to me and may subject me to civil or criminal prosecution under State and Federal law. Standards for eligibility and participation in the SFMNP are the same for everyone, regardless of race, color, national origin, age, disability, or sex. I understand that I may appeal any decision made by the local agency regarding my eligibility for the SFMNP. By signing this, I acknowledge that my total household income is within the Income guidelines: $23,606 for 1 person in the household; or $31,894 for 2 people in the household and that I am 60 years old or older (or will turn 60 by December 31, 2020). 1st Participant Name (Print): Birth Date (Person the checks are for) Signature 2nd Participant Name (Print): Birth Date (Person the checks are for) Signature Address (Print): Telephone Number: County You Live In: Please place check by the most appropriate identifier for each. Ethnicity: Hispanic or Latino Not Hispanic or Latino Please circle the most appropriate identifier for each: Ethnicity: Hispanic or Latino Not Hispanic or Latino Race: American Indian or Alaskan Native Asian Black or African American Native Hawaiian or other Pacific Islander White If more responses are received than funding allows, you will be notified by mail. Mail or email your completed SFMNP form before September 30, 2020: Mail to Area Agency on Aging for Luzerne & Wyoming Counties, 93 North State Street, Wilkes-Barre, Pa 18701 or Email to Rhonda.Adams@luzernecounty.org THIS INSTITUTION IS AN EQUAL OPPORTUNITY PROVIDER. 93 NORTH STATE STREET | WILKES-BARRE, PA Www.luzernecounty.org 80963089