
Advertisement
-
Published Date
June 5, 2022This ad was originally published on this date and may contain an offer that is no longer valid. To learn more about this business and its most recent offers, click here.
Ad Text
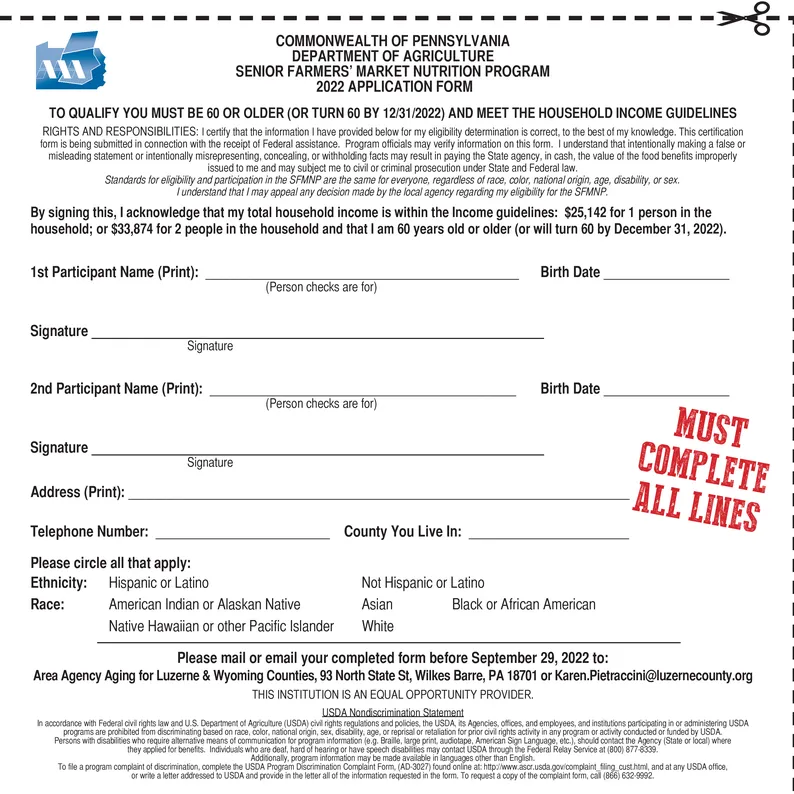
COMMONWEALTH OF PENNSYLVANIA DEPARTMENT OF AGRICULTURE M SENIOR FARMERS' MARKET NUTRITION PROGRAM 2022 APPLICATION FORM TO QUALIFY YOU MUST BE 60 OR OLDER (OR TURN 60 BY 12/31/2022) AND MEET THE HOUSEHOLD INCOME GUIDELINES RIGHTS AND RESPONSIBILITIES: I certify that the information I have provided below for my eligibility determination is correct, to the best of my knowledge. This certification form is being submitted in connection with the receipt of Federal assistance. Program officials may verify information on this form. I understand that intentionally making a false or misleading statement or intentionally misrepresenting, concealing, or withholding facts may result in paying the State agency, in cash, the value of the food benefits improperly issued to me and may subject me to civil or criminal prosecution under State and Federal law. Standards for eligibility and participation in the SFMNP are the same for everyone, regardless of race, color, national origin, age, disability, or sex. I understand that I may appeal any decision made by the local agency regarding my eligibility for the SFMNP. By signing this, I acknowledge that my total household income is within the Income guidelines: $25,142 for 1 person in the household; or $33,874 for 2 people in the household and that I am 60 years old or older (or will turn 60 by December 31, 2022). 1st Participant Name (Print): Birth Date (Person checks are for) Signature 2nd Participant Name (Print): Birth Date (Person checks are for) Signature MUST COMPLETE ALL LINES Address (Print): Telephone Number: Please circle all that apply: Ethnicity: Hispanic or Latino Race: Not Hispanic or Latino American Indian or Alaskan Native Asian Black or African American Native Hawaiian or other Pacific Islander White Please mail or email your completed form before September 29, 2022 to: Area Agency Aging for Luzerne & Wyoming Counties, 93 North State St, Wilkes Barre, PA 18701 or Karen.Pietraccini@luzernecounty.org THIS INSTITUTION IS AN EQUAL OPPORTUNITY PROVIDER. USDA Nondiscrimination Statement In accordance with Federal civil rights law and U.S. Department of Agriculture (USDA) civil rights regulations and policies, the USDA, its Agencies, offices, and employees, and institutions participating in or administering USDA programs are prohibited from discriminating based on race, color, national origin, sex, disability, age, or reprisal or retaliation for prior civil rights activity in any program or activity conducted or funded by USDA. Persons with disabilities who require alternative means of communication for program information (e.g. Braille, large print, audiotape, American Sign Language, etc.), should contact the Agency (State or local) where they applied for benefits. Individuals who are deaf, hard of hearing or have speech disabilities may contact USDA through the Federal Relay Service at (800) 877-8339. Additionally, program information may be made available in languages other than English. To file a program complaint of discrimination, complete the USDA Program Discrimination Complaint Form. (AD-3027) found online at: http://www.ascr.usda.gov/complaint_filing_cust.html, and at any USDA office, or write a letter addressed to USDA and provide in the letter all of the information requested in the form. To request a copy of the complaint form, call (866) 632-9992. Signature Signature County You Live In: COMMONWEALTH OF PENNSYLVANIA DEPARTMENT OF AGRICULTURE M SENIOR FARMERS ' MARKET NUTRITION PROGRAM 2022 APPLICATION FORM TO QUALIFY YOU MUST BE 60 OR OLDER ( OR TURN 60 BY 12/31/2022 ) AND MEET THE HOUSEHOLD INCOME GUIDELINES RIGHTS AND RESPONSIBILITIES : I certify that the information I have provided below for my eligibility determination is correct , to the best of my knowledge . This certification form is being submitted in connection with the receipt of Federal assistance . Program officials may verify information on this form . I understand that intentionally making a false or misleading statement or intentionally misrepresenting , concealing , or withholding facts may result in paying the State agency , in cash , the value of the food benefits improperly issued to me and may subject me to civil or criminal prosecution under State and Federal law . Standards for eligibility and participation in the SFMNP are the same for everyone , regardless of race , color , national origin , age , disability , or sex . I understand that I may appeal any decision made by the local agency regarding my eligibility for the SFMNP . By signing this , I acknowledge that my total household income is within the Income guidelines : $ 25,142 for 1 person in the household ; or $ 33,874 for 2 people in the household and that I am 60 years old or older ( or will turn 60 by December 31 , 2022 ) . 1st Participant Name ( Print ) : Birth Date ( Person checks are for ) Signature 2nd Participant Name ( Print ) : Birth Date ( Person checks are for ) Signature MUST COMPLETE ALL LINES Address ( Print ) : Telephone Number : Please circle all that apply : Ethnicity : Hispanic or Latino Race : Not Hispanic or Latino American Indian or Alaskan Native Asian Black or African American Native Hawaiian or other Pacific Islander White Please mail or email your completed form before September 29 , 2022 to : Area Agency Aging for Luzerne & Wyoming Counties , 93 North State St , Wilkes Barre , PA 18701 or Karen.Pietraccini@luzernecounty.org THIS INSTITUTION IS AN EQUAL OPPORTUNITY PROVIDER . USDA Nondiscrimination Statement In accordance with Federal civil rights law and U.S. Department of Agriculture ( USDA ) civil rights regulations and policies , the USDA , its Agencies , offices , and employees , and institutions participating in or administering USDA programs are prohibited from discriminating based on race , color , national origin , sex , disability , age , or reprisal or retaliation for prior civil rights activity in any program or activity conducted or funded by USDA . Persons with disabilities who require alternative means of communication for program information ( e.g. Braille , large print , audiotape , American Sign Language , etc. ) , should contact the Agency ( State or local ) where they applied for benefits . Individuals who are deaf , hard of hearing or have speech disabilities may contact USDA through the Federal Relay Service at ( 800 ) 877-8339 . Additionally , program information may be made available in languages other than English . To file a program complaint of discrimination , complete the USDA Program Discrimination Complaint Form . ( AD - 3027 ) found online at : http://www.ascr.usda.gov/complaint_filing_cust.html , and at any USDA office , or write a letter addressed to USDA and provide in the letter all of the information requested in the form . To request a copy of the complaint form , call ( 866 ) 632-9992 . Signature Signature County You Live In :